
Photo Gallery | 192822 Views | May 06,2019



May 13 , 2026.
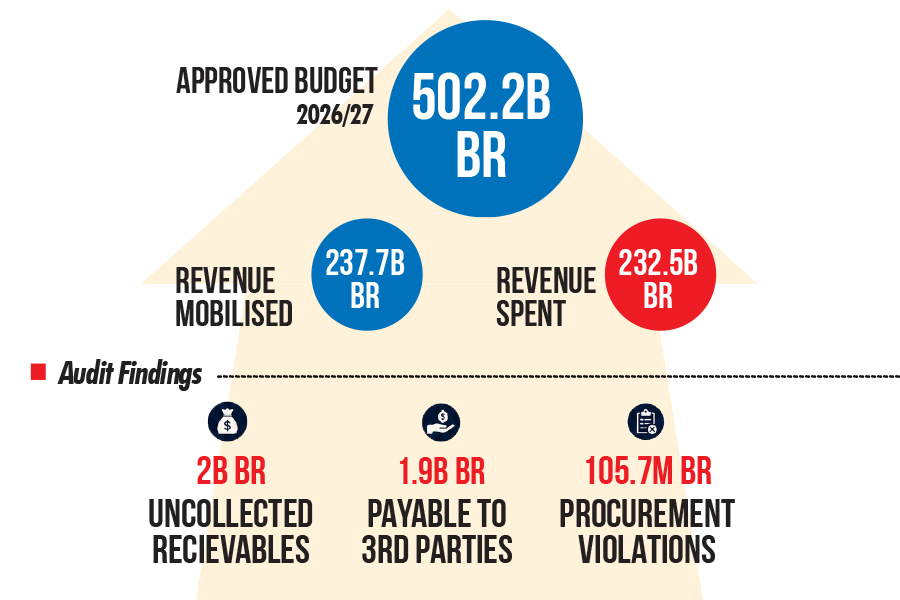
Mayor Adanech Abiebie’s cabinet has approved an additional 9.9 billion Br budget, a midyear patch that lays bare the pressure building inside the city's finances.
Abdulkadir Redwan, the head of city finance bureau, pushed the proposal through after a sudden salary adjustment had already been paid, forcing Adanech's Administration to seek federal subsidy. The supplementary package is anchored by 8.5 billion Br in federal subsidy arrears linked to the wage increase. It also includes 996 million Br in support funds, 451 million Br from improved hospital revenues, and 1.1 billion Br for capital projects.
The remainder is folded into the common budget.
The request marks a reversal for an Administration that entered the fiscal year with a 350 billion Br budget prepared without federal subsidy support. The unplanned wage bill forced the city to return to federal coffers, showing how quickly budget assumptions can shift when salary commitments outpace allocations.
The fiscal pressure has widened beyond payroll. It is both immediate and structural, cutting across wages, legacy debt, construction costs, and an expanding urban population.
Addis Abeba’s housing programme, one of the Administration’s most visible political projects and social commitments, has become a major test of the city’s balance sheet. City officials have moved toward a direct, treasury-funded model after years of restricted borrowing and the partial repayment of the condominium projects' debt accumulated under earlier schemes. Of the total 90 billion Br liabilities for financing condo housing, the city inherited more than 60 billion Br, a burden that froze access to credit from the state-owned Commercial Bank of Ethiopia (CBE). Nearly 30 Bilion Br of the rest of the debt remains outstanding, casting a shadow over the Administration’s housing ambitions.
Mayor Adanech told the City Council on Friday, May 8, 2026, gathered at the Adwa Victory Memorial Museum, that her Administration had delivered 480,000 housing units over the past five years. But annual demand in Addis Abeba exceeds 486,000 units, where nearly 60pc of the nation's residents are believed to live in rental properties.
The City Administration is now overseeing construction of 165,903 housing units across five delivery streams. However, the inherited liabilities remain a drag.
“Due to the previous malfunctioning system, it was unknown who the payer was, but the city Administration was obligated to pay based on the guarantee it had provided,” the Mayor said.
The debt burden has limited access to additional commercial bank financing and sharpened the dilemma facing savers under condominium housing projects, some of whom have waited up to two decades.
“It isn't possible to provide these houses at the price they saved for 15 and 20 years ago,” Adanech told city Councilers.
Thousands of savers remain first in line for allocation. The Houses Corporation is reviewing ways to adjust its contributions to current construction costs. One option under consideration is to use the government’s equity share in Public-Private Partnership (PPP) housing projects as a subsidy, lowering the amount long-term savers would pay when homes are transferred.
The Administration’s delivery framework has shifted from a state-led monopoly to five channels, including public-private partnership projects, individual home builders and private real estate developers.
“The demand is vast, and there are realistic reasons why it can't be fully met at once,” the Mayor told council members, referring to the million-plus backlog of registered condominium savers.
Of the units now under construction, 50,000 are financed directly through treasury allocations, and about 55,000 are under public-private arrangements. To keep prices within reach as construction costs rise, the city Administration says the government’s equity in PPP projects will subsidise long-term savers rather than return to the Administration as completed units.
“We've decided that the government's share in PPP projects will be used to offset prices rather than the city taking possession of the units,” Adanech said.
She disclosed that housing projects in Aqaqi-Qality, Gerji, and Bulbula are approaching completion.
Institutional support has gone to 119 housing cooperatives building 13,630 units on land allocated free of lease fees by the city. Officials are also monitoring 3,273 real estate units and 20,000 individually built homes to keep projects on schedule. The city’s 10-year roadmap targets an annual production capacity of 100,000 units. According to the Mayor, diversified supply channels have helped stabilise Addis Abeba’s real estate market.
The federal government’s 10-Year Development Plan, launched in 2021, targets to see through the construction of more than 4.4 million housing units nationwide by 2030 and raise urban housing access from the current 64pc to 80pc. Addis Abeba bears the heaviest pressure, with a backlog of more than one million registered applicants seeking affordable condominium housing.
Rapid urbanisation is intensifying the shortfall. Population growth in urban centres is projected at 3.8pc to 5.4pc a year. In the 15 years beginning in 2000, Addis Abeba’s population grew by 3.7pc, from 2.8 million residents to 3.8 million. According to World Population Review, the city's population reached 4.2 million this year, registering a 2.3pc annual growth from last year.
Experts argue that the housing shortage has been aggravated by a market dominated by owner-occupiers and fragmented informal rental systems, contributing to overcrowding and deteriorating housing quality. With public financing unable to meet demand, the government has increasingly turned to PPP models and is deploying a multi-billion-dollar framework to increase urban housing availability.
According to Mered B. Fikereyohannes, CEO of Pragma Capital and a finance and investment advisor, the city’s housing and fiscal pressures require structural reform rather than temporary budget fixes. He argued that the housing deficit cannot be addressed through mismanaged condominium systems that ignore the time value of money. For Mered, the “permanent solution” begins with land administration reform.
"Land management must become more efficient or partially privatised so land remains accessible and affordable," he told Fortune.
He also proposed a public company for mortgage refinancing that would issue 20- to 30-year bonds bought by pension funds at competitive rates. The proceeds would be used to purchase mortgage contracts from commercial banks, freeing them from long-term debt exposure and enabling new housing loans.
"These contracts would function as mortgage-backed securities, and the ownership of the refinancing institution should be shared among the government, commercial banks, and pension funds," said Merid.
To reach 12pc of GDP in housing contributions, Mered estimated, the financial sector would need the capacity to issue as much as 2.5 trillion Br in annual mortgage financing, "which is possible only through advanced refinancing and bond-market systems." He argued that the issue is not simply injecting liquidity. Banks create money through lending, but the economy should absorb it through productive activity, such as housing construction and job creation.
Merid argued that the city Administration's return to federal subsidy signalled financial mismanagement. He urged Mayor Adanech's Administration to consider municipal bonds instead, especially for large capital projects such as public housing and corridor development.
"By offering yields above Treasury bill rates, the city could attract pension funds and institutional investors while reducing reliance on federal transfers," said Merid.
PUBLISHED ON
May 13,2026 [ VOL
27 , NO
1359]
Photo Gallery | 192822 Views | May 06,2019

Photo Gallery | 182725 Views | Apr 26,2019

Photo Gallery | 179485 Views | Oct 06,2021

My Opinion | 144968 Views | Aug 14,2021





Aug 8 , 2026
The World Bank asks readers to picture a mother in rural Ethiopia who has never held...

Jul 31 , 2026
Weldu Yiheysh has not read the Pacific temperature charts. He does not need to. In Shibta District of Enderta Wereda, in...
Jul 25 , 2026
Ideally, citizens who have paid income tax all year should not have to reach for thei...

Jul 18 , 2026
Pressed in Parliament on jobs and household incomes, Prime Minister Abiy Ahmed (PhD)...







 Loading your updates...
Loading your updates...