
Featured | Sep 08,2024



Aug 30 , 2025.
For Germans, Otto von Bismarck is first remembered as the architect of a unified nation. However, his lesser-known stroke of statecraft continues to have a lasting impact on the world. In 1883, he introduced the world’s first compulsory health insurance law. For Bismarck, it was not altruism as he sought to curb the rise of socialist agitators by guaranteeing a modest income for workers who were sick or injured. Medical coverage, to him, was almost beside the point.
Ethiopia, 128 years later, turned to community-based insurance for a different reason than ideology. In the late 2000s, too many families were selling cattle, pulling children from schools or sinking into debt to pay medical bills, and too many stayed home and died for lack of access to health services. Faced with grim statistics, the ruling Revolutionary Democrats, some of whose leaders were fans of the German leader, adopted a plan that drew inspiration from Bismarck’s legacy but charted its own course.
The community-based health insurance (CBHI) scheme began quietly in 2011, initially confined to 13 weredas scattered across the highlands and lowlands. The design was disarmingly simple. Each household paid a flat annual premium (currently 1,400 Br, equivalent to less than 10 dollars in last week's exchange rate) and could then visit any public clinic or hospital. The federal government chipped in subsidies and covered the poorest individuals outright. In theory, one modest payment would link millions of rural and informal-sector workers to a safety net.
Ambition soon outran geography. In under a decade, the scheme spread to almost all 832 districts. Close to 32 million people, around a quarter of Ethiopians, are now enrolled. Ideally, they enjoy access to more than 1,900 health centres, nearly 250 hospitals and a small but growing list of private pharmacies to ease drug shortages. Insured patients make more than twice as many trips to facilities as their uninsured neighbours.
Catastrophic out-of-pocket spending, once a grim rite of passage for families facing illness, has fallen among the insured. Total consultations have tripled since 2015, while surveys find that fewer households are pushed into poverty by illness.
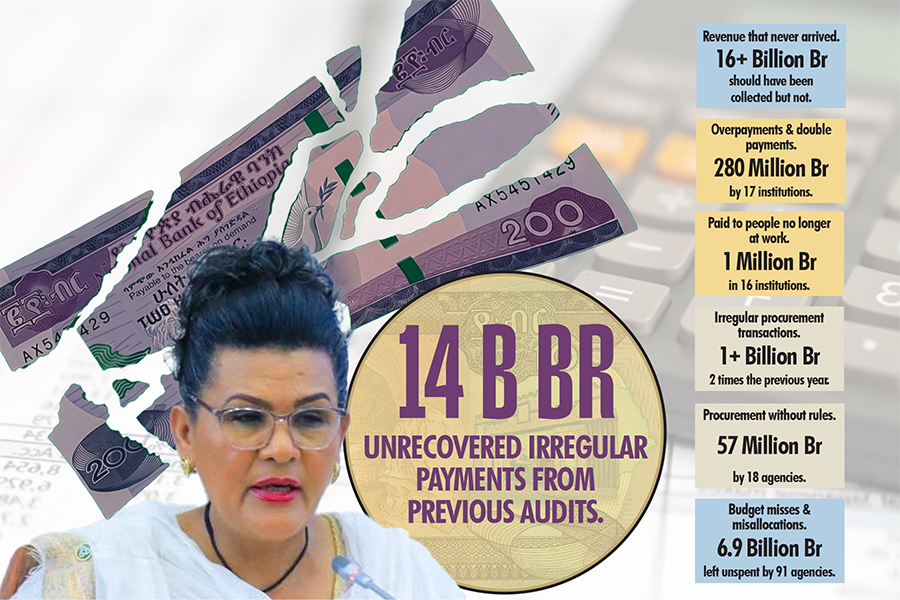
Nonetheless, success masks strain on a national program now estimated to be worth close to 50 billion Br.
The most obvious problem is money. CBHI was deliberately designed with low and affordable premiums, which, although politically popular, may be economically shaky. The annual contribution is well below the actual cost of care. With health needs rising and coverage expanding, the scheme is, in effect, paying out more than it takes in. Last year, for every Birr collected in premiums, the system paid nearly twice as much in claims. The gap is papered over by government subsidies, but with the state budget already stretched thin and donor funding uncertain, this is not a situation that can endure indefinitely.
Already, several district-level schemes have teetered on the brink of bankruptcy.
Participation in the scheme remains voluntary. Young and healthy families often opt out, leaving a pool that is older, sicker and costlier, a textbook case of adverse selection. Renewal rates are around 82pc, but in some districts, one household in five quietly drops out each year.
The flat-rate premium, once praised for simplicity, now distorts incentives. A family of eight pays the same as a childless couple, so larger (and usually poorer) households consume more care for less money. Policymakers tout sliding-scale fees tied to income or head-count, but fear sticker shock. Policymakers who designed the scheme promise broad coverage on a shoestring, a fiscal tightrope that Rwanda avoided by subsidising the very poor and mandating contributions, driving coverage above 80pc.
Geography, too, works against easy solutions. The country is vast, with mountain ranges, deserts, and forests dividing its people. In some regions, health centres are too far away, or too poorly staffed, to be of use. In others, recent conflict or political unrest has disrupted both health service delivery and insurance enrollment.
In well-served districts, enrollment tops 60pc; in remote pastoral areas, it lags badly. In Sidama Regional State, slightly more than one-third of women are insured; in the Central Shoa Zone of Amhara Regional State, the share is nearly double. These disparities uncover deeper inequalities of income, education, infrastructure, and trust. The result is a patchwork of progress and neglect.
Clinics groan under demand. Outpatient visits per member increased from fewer than one per year in 2011 to more than two by 2024. Stock-outs of medicines are routine. There are only 0.2 doctors per 1,000 people, a tenth of Europe’s average.
Insurance survives by pooling risk widely and pricing coverage at or near the actual cost. The domestic insurance pool is patchy, and CBHI will likely stay fragile, and its benefits will be spread too thinly, while its burdens will be borne by those least able to pay.
Officials discuss mandatory enrollment for the informal sector, merging the CBHI with a future social insurance plan for salaried workers, and implementing digital payments to reduce fraud. Pilot schemes test income-based premiums. These are all sensible ideas, on paper. But policy pronouncements are not enough. What the scheme needs now would be a dose of realism, an honest reckoning with its own limits. Premiums should reflect the true cost of care, even if that means politically unpopular increases.
The flat-rate family premium should be rethought, replaced by a system that balances fairness, affordability, and fiscal discipline. Most of all, participation needs to be broadened, ideally, made universal, so that the risks and rewards are shared across the entire population, not the compliant or the unlucky.
The more urgent need is transparency, as data on the scheme is hard to come by. The Ethiopian Health Insurance Agency (EHIA), a federal agency responsible for such a vast task, still lacks a functioning website, which fuels a decline in trust. Insurance, after all, is a social contract. Citizens pay now for protection later only if they believe the system will be there when illness strikes.
Infrastructure should keep pace. More clinics, better equipment, and thousands of extra health workers would help prevent queues from lengthening and drugs from running out. Without that push, insurance risks become a promise honoured in theory, resented in practice.
The lesson from Bismarck’s Germany, and modern peers such as Rwanda, should be self-evident. Universal coverage demands compulsory participation, actuarial honesty and steady investment. Ethiopia has demonstrated that a developing country can enrol millions into a health insurance pool. The question is whether it will fortify the pool before its walls crack.
CBHI has already made illness less ruinous and care more accessible. But it is also a leap of faith teetering on thin financial ice. Raise premiums to match costs, redesign the flat fee, widen the risk pool, and invest heavily in clinics. Policymakers could then demonstrate that collective action can indeed level the odds between town and countryside, as well as between the rich and the poor. Fail, and CBHI may join the long list of well-meant reforms that faltered under the weight of their own ambition.
PUBLISHED ON
Aug 30,2025 [ VOL
26 , NO
1322]
Featured | Sep 08,2024

Fortune News | May 16,2020

Fortune News | Sep 06,2020

Commentaries | Oct 21,2023

News Analysis | May 25,2024

Photo Gallery | 190981 Views | May 06,2019

Photo Gallery | 180764 Views | Apr 26,2019

Photo Gallery | 177435 Views | Oct 06,2021

My Opinion | 143077 Views | Aug 14,2021









Dec 22 , 2024 . By TIZITA SHEWAFERAW
Charged with transforming colossal state-owned enterprises into modern and competitiv...

Aug 18 , 2024 . By AKSAH ITALO
Although predictable Yonas Zerihun's job in the ride-hailing service is not immune to...

Jul 28 , 2024 . By TIZITA SHEWAFERAW
Unhabitual, perhaps too many, Samuel Gebreyohannes, 38, used to occasionally enjoy a couple of beers at breakfast. However, he recently swit...

Jul 13 , 2024 . By AKSAH ITALO
Investors who rely on tractors, trucks, and field vehicles for commuting, transporting commodities, and f...

Jul 7 , 2026
The health sector remains underprovided despite rising public spending, Prime Ministe...

Jul 7 , 2026
Prime Minister Abiy Ahmed (PhD) delivered one of his bluntest rebukes yet to the coun...

Jul 7 , 2026
Prime Minister Abiy answered his critics with a mix of gratitude and edge, thanking l...

Jul 7 , 2026
A ruling-party lawmaker, Mohammed Ahmed, called the Chamber to its feet for Prime Min...













 Loading your updates...
Loading your updates...